Breaking the FGM Vice in Kenya: The Social, Economic and Environmental Viewpoint
Female Genital Mutilation remains a critical global concern, affecting millions of women and girls across continents and reflecting deep-seated gender inequality.
The World Health Organization classifies Female Genital Mutilation (FGM) into four main types. Type I involves the partial or total removal of the clitoris. Type II involves the partial or total removal of the clitoris and the labia minora, with or without removal of the labia majora. Type III, commonly known as infibulation, involves narrowing the vaginal opening by creating a covering seal. Type IV includes other harmful procedures such as piercing, pricking, scraping or cauterisation.
These classifications help health professionals, policymakers and communities understand the scope, nature and severity of the practice.
Recent reports from the United Nations and the World Health Organization indicate that approximately 50% of the total progress made in reducing FGM since 1990 has occurred within the last decade. This trend suggests that sustained advocacy, community-led education, legal reforms and global awareness campaigns are yielding measurable results.
FGM at a Glance
| FGM Component | Statistic |
|---|---|
| Estimated number of women and girls who have undergone FGM globally | 230 million |
| Types of FGM under the WHO classification | 4 |
| Number of countries where FGM is prevalent | More than 30 |
| Age range within which girls are most vulnerable to FGM | Birth to 15 years |
| Estimated number of girls currently at risk of undergoing FGM globally | 4 million |
| Current probability of a girl undergoing FGM compared with 1996 | Approximately 30% of the 1996 probability |
| Main geographical regions where FGM is prevalent | Africa, the Middle East and Asia |
| Countries where more than half of affected women and girls live | Egypt, Ethiopia, Indonesia and Sudan |
| Common short-term physical consequences | Severe bleeding, infection, physical trauma and death |
| Common long-term physical consequences | Chronic pain, cysts, infertility, obstetric complications and increased risk of newborn loss |
| Common long-term psychological consequences | Depression, anxiety and post-traumatic stress disorder |
| Number of countries with laws criminalising FGM | Approximately 70 |
At the continental level, Africa bears the highest burden of FGM globally, with diverse cultural, economic and social factors sustaining the practice. Within East Africa, countries such as Kenya demonstrate significant differences in prevalence, illustrating how local norms interact with national laws, education and interventions.
Trends in FGM Among Girls Aged 0–17
Available evidence shows a general decline in FGM among girls aged 0–17 from the mid-1990s to the 2010s. However, the rate and consistency of this decline differ considerably across countries and regions.
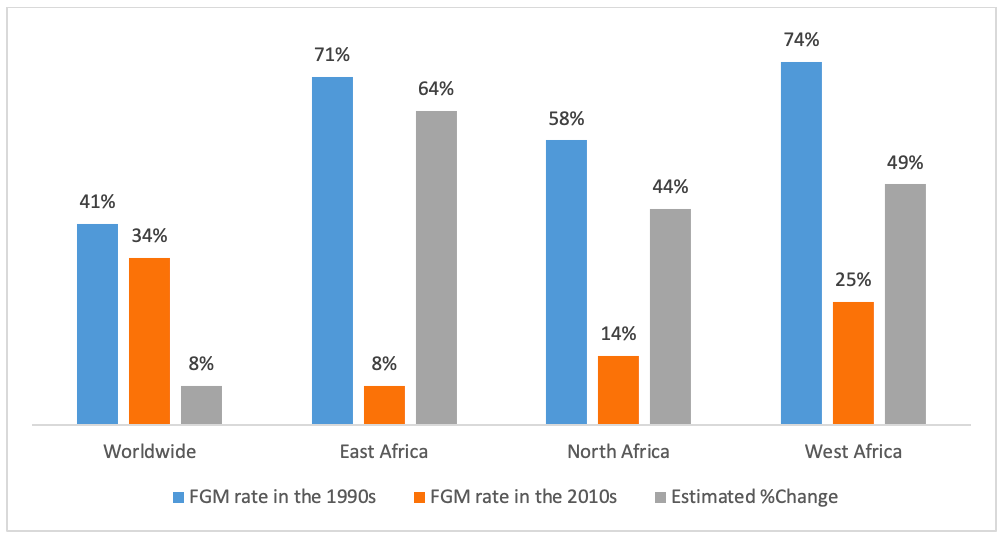
Figure 1: Changes in the prevalence of Female Genital Mutilation among girls aged 0–17 from the mid-1990s to the 2010s.
Despite the recent decline in FGM among younger generations in several countries, the total number of FGM survivors increased considerably during the 1990s and early 2000s. This increase was largely driven by rapid population growth in countries where the practice remained prevalent.
Several parts of North and West Africa have recorded significant reductions in FGM prevalence. Progress has, however, been comparatively slow in some other regions. In certain parts of Western Asia, prevalence among children has remained unchanged or has increased over time.
Even in countries where legislation criminalising FGM is in place, enforcement remains uneven. Tangible progress at the community level does not always correspond with legislative reforms. These dynamics underscore the need for sustained and context-specific strategies that go beyond legislation to address underlying social norms and demographic pressures.
Legal frameworks are essential, but without consistent implementation, monitoring and local engagement, their impact remains limited.
FGM in East Africa at a Glance
Approximately 42 million girls and women in East Africa, particularly those aged between 15 and 49, are estimated to have undergone FGM. This represents approximately 20% of all FGM cases reported globally.
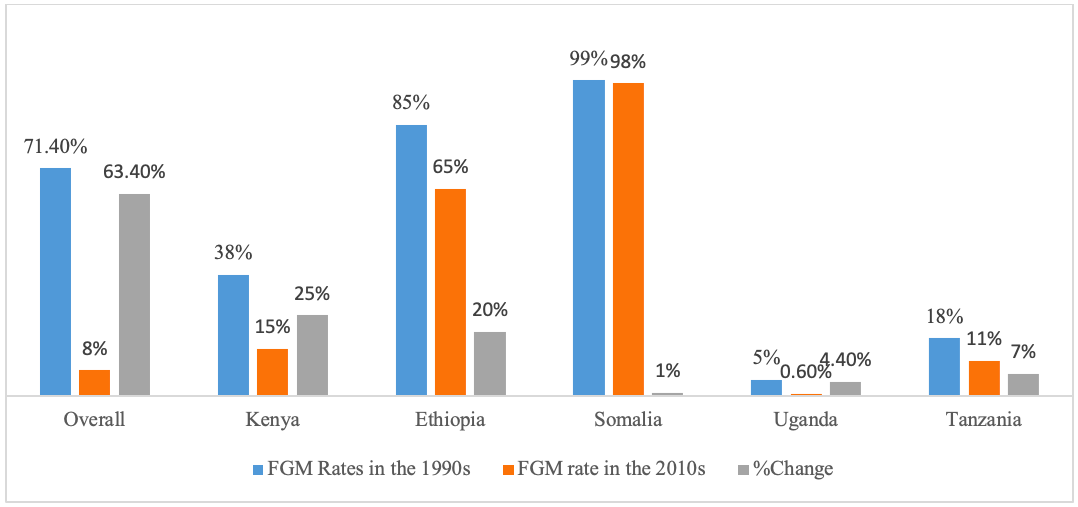
Figure 2: The prevalence and regional distribution of Female Genital Mutilation in East Africa.
FGM Among Children and Adolescents in East Africa
Over the past two decades, the prevalence of FGM among children has declined dramatically in East Africa. In pooled regional data, prevalence among girls aged 0–14 declined from approximately 71% in the mid-1990s to about 8% by 2016.
Younger groups, including girls aged 0–14 and 15–19, consistently show steeper declines than older women. This reflects gradual but meaningful changes in community attitudes and social norms.
The sustained reduction over approximately 20 years suggests that community engagement, strengthened legal frameworks, improved access to education and persistent advocacy are contributing to the abandonment of the practice.
FGM Among Adults in East Africa
Adult FGM prevalence remains high in several East African countries because older generations of women were subjected to FGM before anti-FGM campaigns became widespread.
In Ethiopia, for example, approximately 65% of women aged 15–49 have undergone FGM, illustrating the long-term legacy of the practice. In Somalia, prevalence remains almost universal at approximately 99%, making it one of the countries with the highest FGM rates globally.
These differences highlight both the progress achieved among younger generations and the substantial challenges that remain in eliminating FGM within East Africa.
A Focus on Kenya
Despite sustained campaigns against the practice, FGM continues among several communities in Kenya. National prevalence data reveal clear generational differences.
Among young women aged 15–19, approximately 9% have undergone FGM, compared with about 23% among women aged 45–49. This generational difference indicates that the practice is declining, although it has not been eliminated.
Traditional practitioners continue to conduct most FGM procedures in secrecy. These practitioners account for approximately 82% of reported FGM cases among women aged 15–49. A smaller proportion of the procedures is performed by healthcare workers, contributing to the medicalisation of FGM.
The most commonly reported form of FGM in Kenya is Type II, which involves the partial or total removal of the clitoris and labia minora, with or without removal of the labia majora. This form accounts for approximately 70% of reported FGM cases in Kenya.
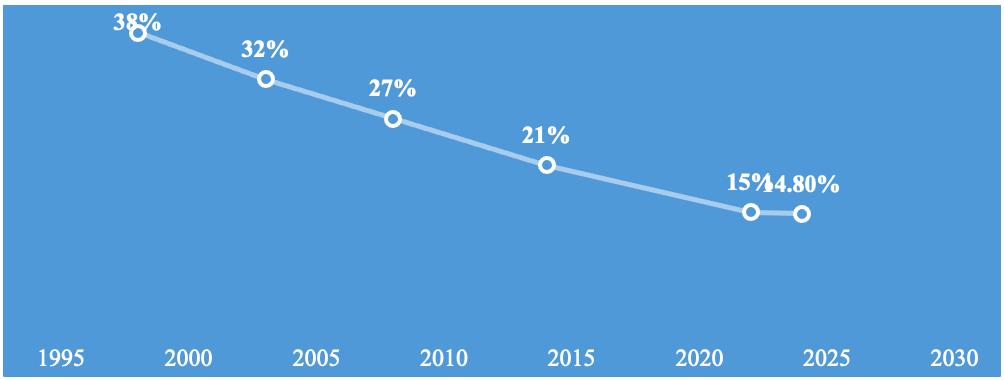
Figure 3: Generational differences in Female Genital Mutilation prevalence among women and girls in Kenya.
The gap between younger and older age groups highlights a gradual decline over time, reflecting changing social norms, improved awareness, increased access to education and sustained anti-FGM advocacy.
Regional Differences in FGM Prevalence in Kenya
Despite the substantial progress achieved through anti-FGM campaigns, significant regional disparities persist. Most FGM procedures are conducted when girls are between 5 and 14 years old, with nearly 45% reportedly taking place between the ages of 10 and 14.
In Kenya’s North Eastern region, prevalence among women aged 15–49 is approximately 97%. County-level data indicate similarly high rates in Mandera at approximately 96%, Marsabit at 83%, Kisii at 77% and Samburu at 76%. Busia records one of the lowest prevalence rates at approximately 0.1%.
Variation among ethnic communities is also pronounced, with relatively high prevalence reported among Somali, Kisii, Maasai and Samburu communities.
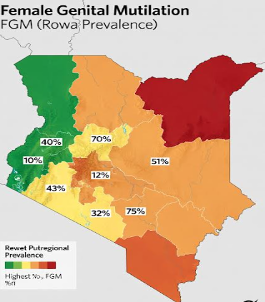
Figure 4: Regional and county-level variations in Female Genital Mutilation prevalence across Kenya.
Why Does FGM Persist in Kenya?
Anyone seeking to contribute effectively to the elimination of FGM must remain open-minded enough to understand its underlying causes. Doing so can replace the illusion of a single “magic bullet” with more realistic, culturally informed and practical interventions.
FGM is sustained by multiple and interconnected social, cultural, economic, psychological and environmental factors. A rigid or one-dimensional approach may generate resistance, secrecy and community backlash. Existing literature identifies several reasons for the persistence of FGM among communities where it continues to be practised in Kenya.
FGM as a Marker of Identity and Marriageability in North Eastern Kenya
In Wajir, Garissa, Mandera, Marsabit and the wider North Eastern region, FGM remains deeply embedded in social life. Some communities have normalised the practice as a marker of identity, family honour and eligibility for marriage.
Families that refuse to conform may experience strong social sanctions. Within some Somali communities, FGM is regarded as an important rite of passage associated with womanhood, respectability and family honour.
Although prominent religious leaders have clarified that FGM is not a requirement of Islam, perceived religious justifications persist and continue to reinforce the practice among some households.
Regional Isolation and Cross-Border Community Ties
Geographic isolation, inadequate infrastructure and inconsistent law enforcement can facilitate the continuation of FGM by making detection and intervention more difficult.
Communities in North Eastern Kenya also maintain strong cross-border relationships with communities in Somalia and Ethiopia, where FGM prevalence remains high. In this context, the practice may be viewed as an expression of cultural solidarity and continuity among neighbouring communities with shared ancestry and traditions.
FGM and Cultural Traditions in Western Kenya
FGM continues in Kisii, Nyamira and parts of the Kuria region in South Nyanza. As in some Somali communities, long-standing cultural traditions associate the practice with womanhood, maturity, respectability and family reputation.
Intergenerational transmission of cultural norms, combined with peer pressure and community expectations, continues to encourage the practice.
In some areas, medicalisation has emerged, with healthcare providers performing FGM under the mistaken assumption that it is safer when conducted by health professionals. This has unintentionally legitimised the practice and created a significant barrier to elimination efforts.
Culture and FGM in the Rift Valley and Eastern Kenya
Among Maasai, Samburu and other pastoralist communities in Isiolo, the Central Rift and the North Rift, FGM is intertwined with cultural values related to honour, fertility, marriage and transition to adulthood.
In some Maasai communities, particularly in Kajiado and Narok, FGM is still perceived as necessary for marriage eligibility and social respect. To avoid prosecution, some families conduct ceremonies secretly or seek medicalised procedures.
In Tana River, the practice persists partly because it continues to be viewed by some groups as a marker of cultural identity and womanhood.
Climate Change and FGM in Arid and Semi-Arid Areas
Climate shocks, including drought, livestock loss, food insecurity and displacement, intensify household economic vulnerability in Kenya’s arid and semi-arid regions.
Under such conditions, some families may view early marriage and bride price as coping strategies. Where FGM is considered a prerequisite for marriage, economic hardship can increase pressure to subject girls to the practice.
In these circumstances, FGM becomes indirectly linked to climate vulnerability because it is perceived as improving a girl’s marriage prospects and providing the household with financial or social support.
Legal prohibition has, in some cases, pushed the practice underground, making it less visible without necessarily eliminating it.
Regions Where FGM Prevalence Is Lowest
FGM prevalence is comparatively low in Busia and other parts of Western Kenya, Nairobi and much of Central Kenya.
Lower prevalence in these regions is often associated with higher literacy levels, urbanisation, increased access to education, alternative economic opportunities and greater awareness of legal protections for women and girls.
Nevertheless, isolated cases continue to occur because of residual cultural beliefs, migration and localised social pressure. This demonstrates that even in low-prevalence regions, continued vigilance and sustained community engagement remain necessary.
Concluding Remarks
FGM remains prevalent in parts of Asia, the Middle East and Africa. Within East Africa, Kenya, Ethiopia and Somalia continue to bear a substantial share of the regional burden.
In Kenya, the practice is most prevalent in North Eastern counties such as Wajir, Mandera and Garissa; in Marsabit and Isiolo; in sections of the Central and South Rift, including Narok, Kajiado and Samburu; in Tana River; and in southwestern areas such as Kisii, Nyamira and Kuria.
FGM continues despite legal prohibitions and numerous interventions intended to eliminate it. Culturally, the practice is reinforced by entrenched social norms, intergenerational expectations, psychological pressure relating to identity and social acceptance, marriageability and perceived religious obligations.
Economic hardship and environmental pressures, including drought, livestock loss and resource scarcity in pastoralist communities, can further exacerbate the practice by encouraging early marriage as a household coping strategy.
These intersecting social, cultural, psychological, economic and environmental factors make FGM a complex challenge. Eliminating the practice therefore requires integrated and multidisciplinary interventions involving education, legal enforcement, livelihood support, climate resilience, survivor services, religious leadership, youth engagement and locally led transformation of social norms.